THE PURELY PALATINE APPROACH.
I’ve already talked about the clinical crown lenghtening but I want to talk about that again, since it’s a kind of surgery that happens in a dental practice on a daily basis.
Today I want to show you a variant in the technique.
There are few things I remember from Uni; of course, I retain the basics of dentistry, but I remember clearly very few specific pieces of information. I can still hear one of this loud and clear in my mind, though. I remember chasing my Endodontics professor to the vending machines as if it were yesterday, to make sure I understood
well…and he said:
“when you reconstruct a devitalized back tooth you must cover the cusps”.
A staple of my basic dentistry.
I know that if the walls have a specific thickness (I think 3 mm) you cannot protect that area. But I won’t discuss this, because it’s definitely not my field.
I am a surgeon and to me, basic information is enough:
DEVITALIZED TOOTH>>>PROTECT CUSPS
“Yeah, but we all knew this! It took you 13 lines to repeat something that is obvious to everybody!”
The problem is that in our daily practice, we keep running into endodontically treated posterior teeth that are FRACTURED.
At least two patients a week come in emergency with a coronal fracture, that is often extended to the root.
I don’t know why, but really, countless colleagues keep devitalizing teeth and then perform a filling on top of it. MOST TIMES leaving leftovers from the preexisting filling and only “corking” the access cavity.
Stefano an I must have seen no more than 30 onlay/overlays in six years, in our about 9000 patients’ , mouths.
In the hundreds devitalized teeth we have found only CROWNS (this one, more rarely) or FILLINGS without an adequate protection of the cusps. We often find two or three different materials in the same tooth
(when there’s also a dentatus post!)
Here it is:
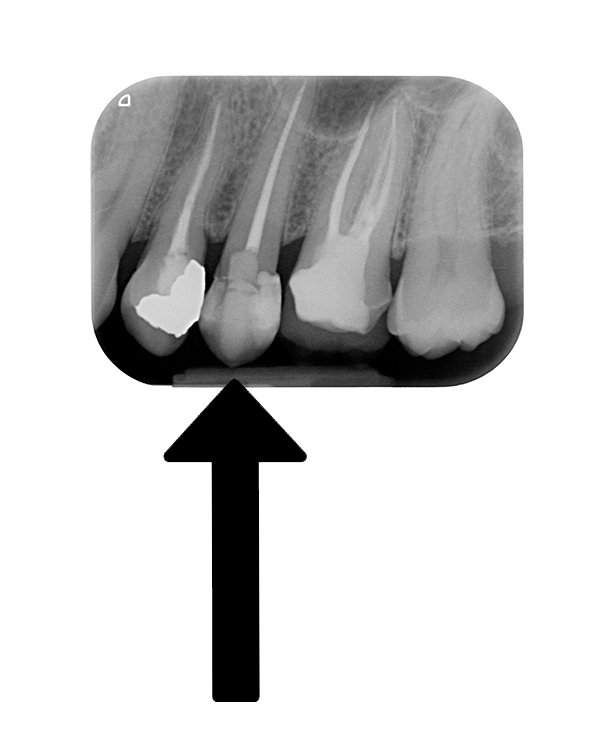
The inlay on 2.6 is ours (the canal treatment isn’t!! Not retreated, because there wasn’t a lesion…)
Look at the leading actor: posterior, endodontically treated, UNPROTECTED and…filled with tree different composites. A mesial one, a distal one and one for the “canalization”!
What can you expect from a tooth like this? I wonder what the colleague who did it was expecting.
I’ll tell you what:
“I’ve always done so and I’ve never broken one.”
Actually, my friend, almost all of them break, but patients don’t come back to your practice, so you don’t see them.
Here’s what happens:


Coronal fracture complicated by a subgingival fracture margin of at least 3 mm.
Premolars and molars often fracture on the palatine side. In these cases, we can perform a crown lenghtening limited to this aspect, so that we preserve the buccal esthetics while keeping the essential condition of a positive anatomy in the scalloped gumline.
Here’s a video explaining this technique, completely for free.
If you like the video subscribe to our newsletter to stay tuned.