"Midway in the journey of our life I came to myself in a dark wood, for the straight way was lost"
My working week has always ended on Saturday, not on Friday. So it is on Saturday that I run in the classic “Friday night’s last case”, which is always tricky, as we all know.
Last Saturday was no exception, and my agenda surprised with a 1.7 tooth retreatment which, starting from the pre-operative radiograph, made my jaw drop.

Can you see that mesio-buccal canal? From experience, I know that (taking for granted that he is not an incompetent doctor who cannot practice cheap football jerseys China endodontics) if the dentist who treated the patient before me manages to get in apex on two canals, but gets lost before the curve of a root, two problems may have occurred:
- He took a wrong path because of a calcified canal, or he made a mistake in locating the access to the pulp chamber
- He fractured an instrument and couldn’t penetrate further.
In this case, the patient informed me that my colleague had told him that she hadn’t managed to get to the end of a root, so at least she knew what she had not been able to do. Based on most of the pathetic treatments that have been carried out in the mouth of the patients who come here for the first time, I believe my forerunners don’t have the faintest idea of how to carry out a correct canal treatment.
So what’s the best strategy to deal with these cases?
First of all, think it over, before you rush and retreat the tooth; explain to Cheap Elite Jerseys – Wholesale NFL Jerseys Free Shipping From China your patient what Cincinnati Bengals jersey youths you’re expecting to find and what difficulties might occur. This way, if you didn’t manage to do much better than your predecessor, you could still manage to turn your failure in a “success” in the eyes of your patient.
Let me rephrase this better.
To this patient here, I said: “Alright, so this tooth might be difficult to treat in one of the roots. If you look at the x-ray, you can see this white material, which should get to the end of the tooth, as in the other two roots (and I point at the monitor). Can you see that it just gets to the half of the root? The problem is that, when a dentist stops before a big curve (and here I point at the mesio-buccal shape of the curve), he might have pierced the root or he might make us pierce it, if we follow his path; or he might Pittsburgh Steelers jerseys have fractured one of those instruments we generally use to go through the nerve canals of the tooth, failing to negotiate the canal. Now let’s see if, using a microscope, we manage to see what’s happened…Maybe we’ll get to the end of the root right away and I am just overthinking it…the problem is that the infection you have under the tooth is due exactly to that root, so if we don’t fix it, we’ll run the risk of having to remove the lesion under the tooth surgically…”
At this point, the patient has understood that the job could be tough, he senses that you know what you are doing and you have covered your ass in case of a possible failure. After all, you’re not the one who’s made a mess in your patient’s mouth and your role is just analyzing it, and possibly fix it. Canal treatments can be difficult in a vergin tooth. When you can’t carry out the treatment at your best the first time around, if you try the second time with gutta-percha or other materials, calcifications that have worsened overtime, possible fractured instruments or false paths, things cannot but get worse, and it is fair for the patient to know that we’re just trying to get right what someone else has previously screwed up, having to solve more problems than our predecessor had to.
Now it’s time to decide if a pre-operative X-ray is enough or we need a Cone Beam.
I myself choose to do a pre-operative CBCT when I suspect the presence of accessory root canals or to retreat external resorptions. In these cases a CBCT helps me to find what I’m looking for right away.
Still, in cases like this a CBCT is useless, because the gutta-percha present in the canals creates obstacles, and in any case seeing that the gutta-percha pushes on the root contour won’t necessarily help you sort out the situation. Besides, we might also unexpectedly find our way effortlessly, in which case we would have just X-rayed our patient for nothing.
So, let’s start the retreatment.
Palatine canal: easy peasy.
Distobuccal canal : easy peasy.
Mesiobuccal canal: there’s a wall.![]()
Then I try to correct the opening axis of the tooth. Nothing happens.
I just check if the one I’ve found may possibly be a fourth canal and the obstruction a 90 degrees confluence with an MV canal that hadn’t been found previously. Always keep your brain active and consider every possible angle, remember. Still, nothing.
I’ll take an endodontic ultrasonic tip like the one below.
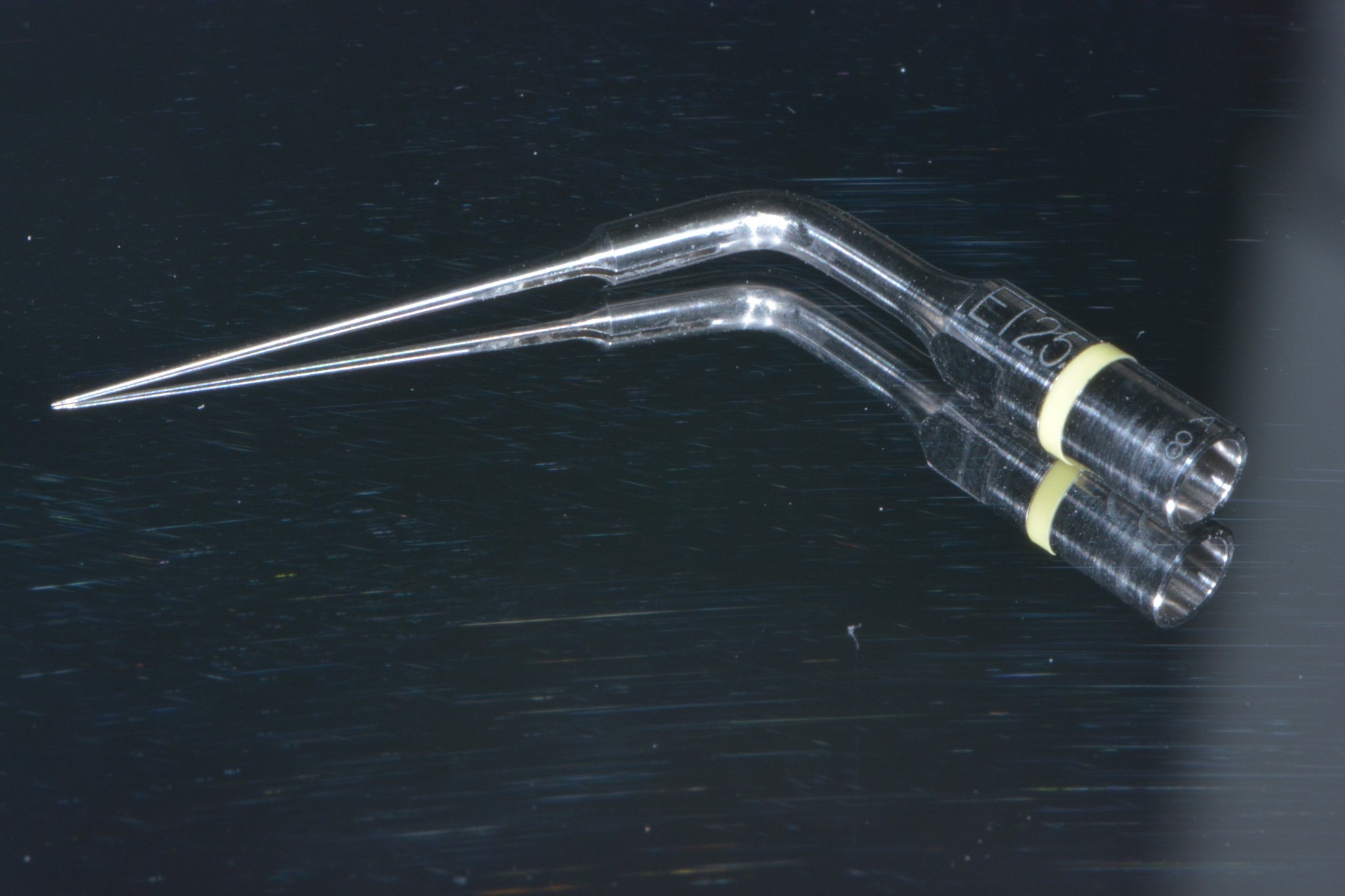
I try to enlarge the canal a bit, to understand if there’s a fractured instrument, moving distally, given the curve is in that direction. Sometimes, the canal opening has just not been corrected, forcing the files to take the wrong path. After this maneuver, I go a little deeper, I suddenly feel an empty space and I tell the patient: “ok, let’s see if we’re there yet, or if we’ve ended up deep down, as I feared.” I use the apex locator, and it rings at 12 mm rather than 20.
“Ok, as I was fearing, we are likely to have ended up off the right path, let’s just have an X-ray taken to understand where we are…”
And here’s the X-ray.

At this point, the patient isn’t worriex because what is happening is exactly what you had predicted, so he understands that the situation is difficult, but you know what you are doing.
Knowing that I proceeded mesially, I forget about that path, and through the ultrasound I create a small room in a distal direction. I try a couple of times with ultrasounds and then files, but still nothing. Ok, so this is the moment when we want to understand a bit more, because we can’t risk on turning the root into Swiss cheese.
Now I am going to perform a 3D scan of your tooth because we need to understand where we’ve ended up, whether there is a canal or not, how the root curves and if the lesion is due to that root, because if we discovered that the canal didn’t exist at all because it’s completely calcified, and that under the root there were no infection, then closing the false path and stopping wouldn’t be a problem.”
We are providing logical explanations, and the patient understands that we have a precise strategy. Moreover, he has never seen a doctor who works with a microscope and has all these means at his disposal. He probably remembers a dentist who didn’t even have magnifying lenses and who surrendered after 10 minutes in a sweat.
Now we’ve green bay jersey cheap got the CT scan results and we can discuss them together.
Once I start working again, using the same endodonic tip that I had used previously, I make my way from where I had created the explorative room in disto-palatine direction. Ideally, I should find a pretty accessible canal without having to advance too much. 15 seconds, with an endodontic tip. I find a file…I feel it crack…Pounding heart…I use the locator…12 mm, 14 mm, 16 mm…19 mm! Ring ring ring! Awesome! Now I’m sure this is the right canal, given it is as long as the disto-buccal one, and I manage to figure out the disto-palatine curvature that I had been expecting.
Both we and the patient are greatly relieved. After this last attempt, we would have been envisaging an apicectomy, that he wanted to avoid and I would have had a hard time performing because of its unfavorable position.
I don’t even carry out the double-check X-ray to make sure that I am in the root. The patient has has been X-rayed long enough today.
I assume that the false path is so small that it can be considered just like a perfectly disenfected lateral canal, so I can rely on gutta-percha for closing it.
Instrument, irrigation and filling using Thermafil.
Voilà.
To enjoy my well-deserved satisfaction, I wait with my patient for my assistant Anna to develop the final X-ray, to have a look at it together.

The result is self-explanatory, and the patient can see for himself that he is in good hands. He’s found a professional he can rely on and he regards his expense as worth the therapy,considering the two hours spent on it, the instruments used, the skills and the competence showed.
Let’s draw our conclusions from this story.
Before rushing on a re treatment, always analyze that your predecessor did wrong and anticipate the difficulties you might have to face. Talk about it with your patient. Find a strategy and stick to it.
Then, a little tip. You might want to treat a case like this with goggles and coaxial light, but, trust me, it’s hard even if you have some chances to succeed. It could be done by an expert who’s been used to operating with a microscope for years. Not by an inexperienced professional who’s just started to use the goggles and doesn’t do much endodontics.
Advanced endodontics must be carried out through a microscope and a CBCT. If you don’t have this technology, but you’re interested in endodontics, make sure you buy it.
If you can’t afford it, or you don’t want to go mad working on these cases, do your patient a favor: send him to an endodontist when you start treating your first false path. Don’t try to be a hero at you patient’s expense or, even worse, scratch the tooth and place an implant tricking the patient into thinking that his tooth couldn’t be recovered due to the first (bad) treatment.
If you know what you need to look for and you see it tank to a CBCT first, and then a microscope, these are complex cases, but not impossibile ones. And, more importantly, they can be solved without resorting to an extraction.