The external root resorption is, in my opinion, a phenomenon many dentists are not even aware of.
Let alone capable of treating it properly.
Hoping you are one of the colleagues who knows what I am talking about, let me briefly introduce the topic to everybody else.
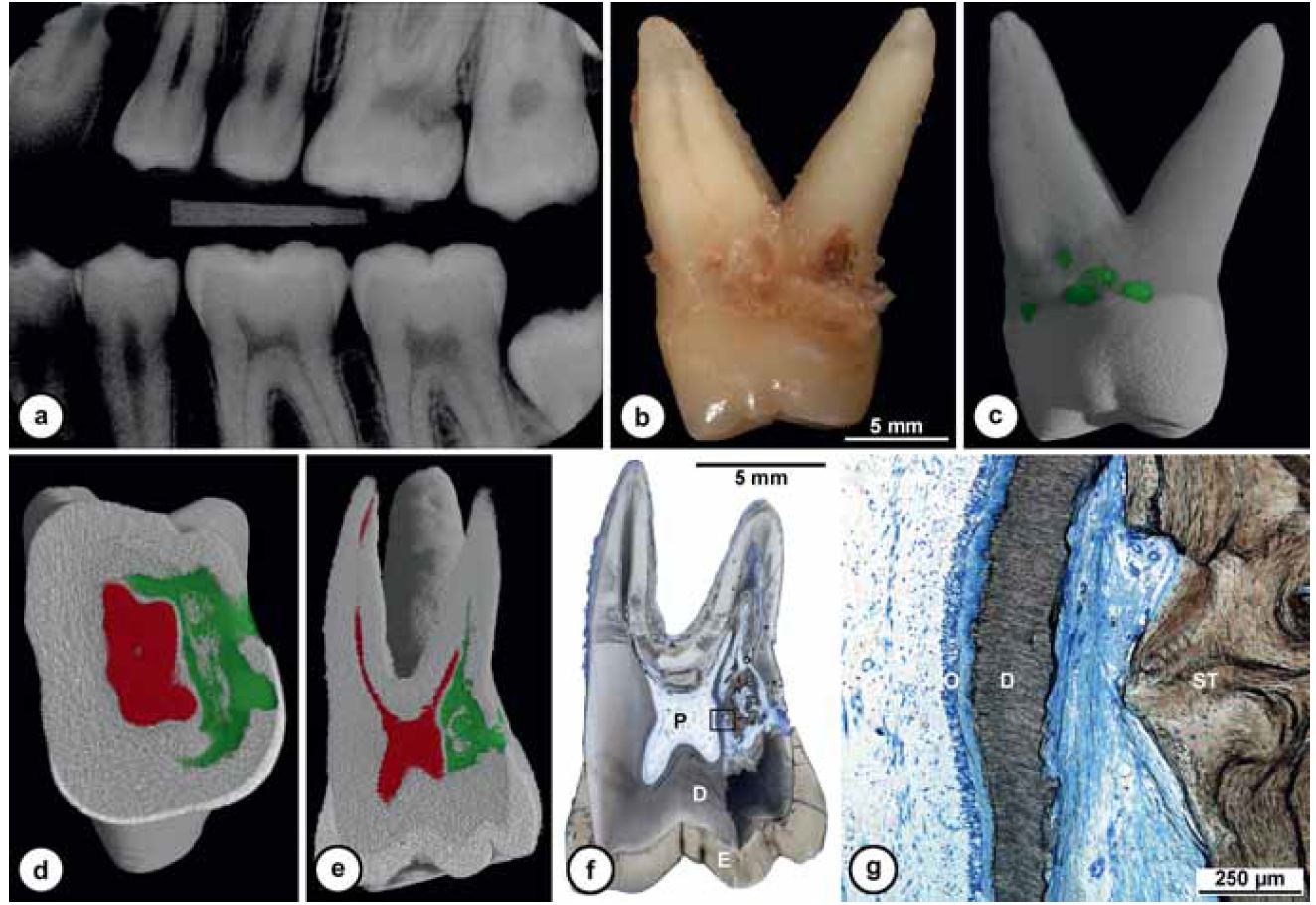
Although the reason why this happens is still unknown, sometimes teeth develop an inflammatory reaction for which, starting from the cervical margin of the tooth, a granulation tissue substitutes dental hard tissue by osteoclasts.
It looks like all this happens because of a damage occourred at the amelocemental junction, and this happens concurrently with:
- traumas
- endodontic bleaching
- orthodontics
- surgical periodontal therapies
Although some etiologic hypotheses exist, the ones above are the main correlations found in external resorption patients’ medical history.
But what happens exactly to teeth affected by this phenomenon?
Basically, some bleeding tissue is created, clinically similar to a bone in a long-standing process, or to a nervous tissue in “younger” teeth, taking over the dentin.
I want to tell you how I discovered what an external root resorption was, clinically.
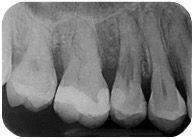
Yeah, because now I’m acting all cool, but back in 2011, a patient having this tooth shows up.
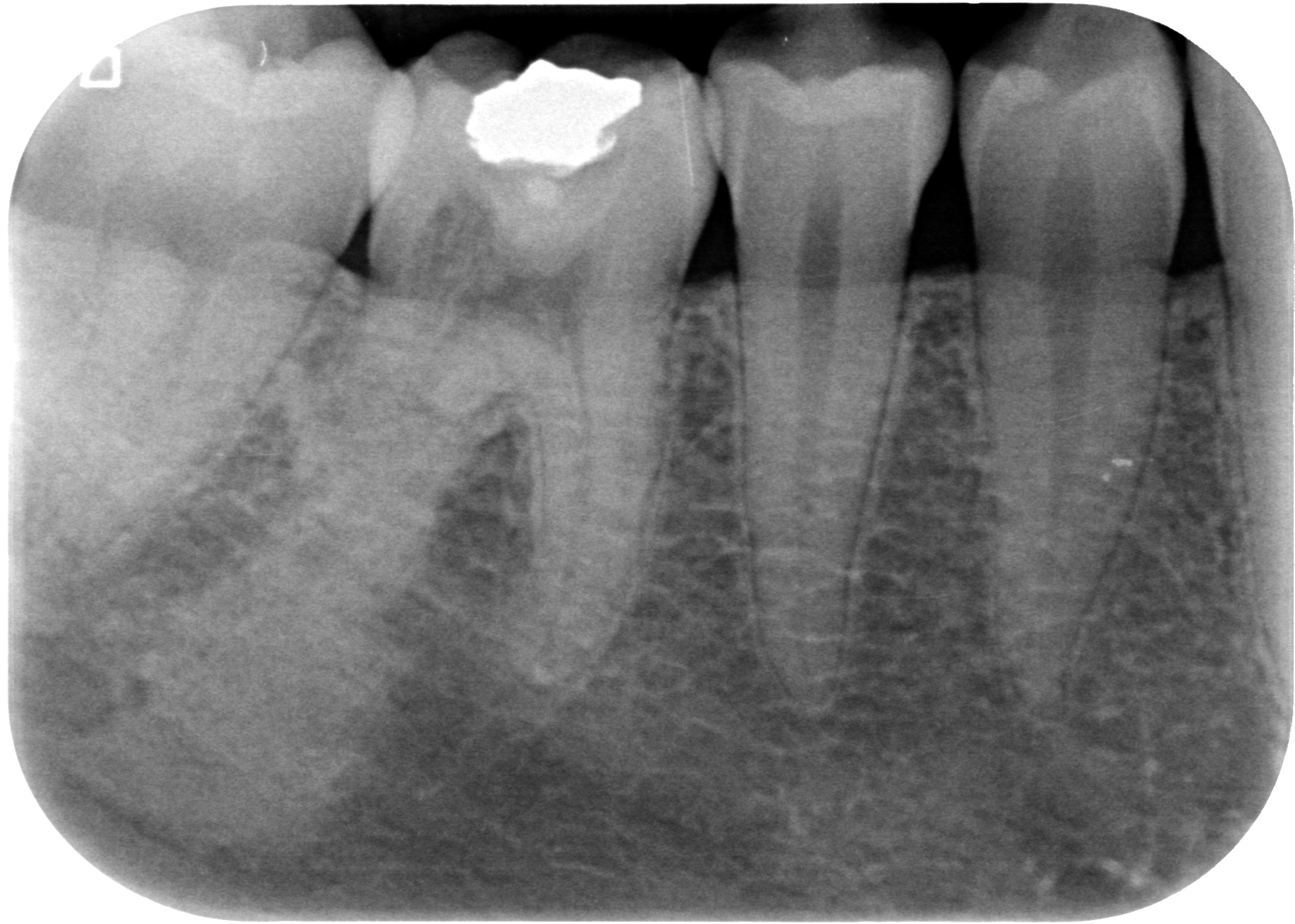
This was my reaction.
What the heck had happened to that tooth!?! Pretty alarmed, I showed the X-ray to Federico, my business associate, and he also thought it was something really bad. Who knows, like one of those absurd tumors we had only studied in radiology books, that had weaseled its way in this 4.6 tooth! What did I come up with, then? An explorative cavity and a biopsy of that tissue!
When I opened the cavity as if to perform a filling, to my great surprise, the tooth has bleeding where there was supposed to be dentin…! and it wouldn’t stop…???
 With a spoon, I took a sample of that misterious tissue, that I thought had probably been implanted there by some aliens during the poor patient’s sleep; after doing this very gently, I kept digging until I could, looking for some healthy tissue, but I had a hard time understanding if I was touching the nerve or that bleeding kept coming from the tooth.
With a spoon, I took a sample of that misterious tissue, that I thought had probably been implanted there by some aliens during the poor patient’s sleep; after doing this very gently, I kept digging until I could, looking for some healthy tissue, but I had a hard time understanding if I was touching the nerve or that bleeding kept coming from the tooth.
I didn’t want to resort to a devitalization, because I wouldn’t have known how to carry it out successfully, without a distal root; so I placed a composite filing.
After a week, the patient was asymptomatic and the test results were ready.
I thought the diagnosis could be something like a tooth carcinoma or a tissue of unknown origins, probably alien.
Instead the verdict was:
“fragments of sclerocalcific tissue”
I think the histologist hadn’t understood much more than I had.
After 5 years, the girl still has an asyntomatic tooth and the X-ray shows that the process stopped.


This happened because, unknowingly, I carried out a correct therapy for a problem I didn’t even know. I removed the granulation tissue as best as I could, stopping or slowing down the process of destruction of the tooth.
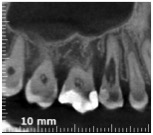
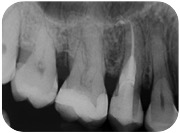
When this case was submitted to my attention, in 2013:
I recognized the same phenomenon I had observed in the abovementioned girl infested with the alien tissue, and I suddenly remembered that cheap nfl jerseys at Uni we had learned about external root resorptions.
So I studied the phenomenon and I was able to make a diagnosis.
That was an external resorption of class IV.
In 1999, in fact, Heithersay classified external root resorptions in four classes (Heythersay, 1999):
- class 1 presents with a little resorption in the cervical area, with a superficial dentin penetration;
- class 2 presents with a well-defined resorption, which penetrated near the pulp chamber with little or no extention to the root dentin;
- class 3 presents a resorption extended in the coronal third of the root;
- class 4 identifies invasive and extended root resorptions, which go beyond the coronal third of the root.
Perfect.
The treatment included removing the granulation tissue surgically or with an orthograde approach and filling the tooth with composite material, as if it were a cavity filling, in class 1 and 2 cases (it is often necessary to combine this procedure with a root canal treatment and a clinical crown lengthening. In class 3 or 4 external resorption the lesion is often filled with MTA, given it often communicate with the periodontium (so far I’ve used Biodentine, but we’ll discuss this in a further post).
Ooooook. Just when I was ready to start, this time well-aware of what cheap jerseys nfl I was about to do, I read that Heithersay recommended not to treat class 4 external root resorptions, because the success rate was 12,5%!!!! (Heithersay, 1999)
But could I possibly think of extracting a seemingly healthy tooth, that had a purely aesthetic function for my patient (who was, in the meantime, wearing an invisible brace)?
Of course not.
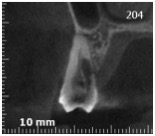
So, to get a deeper understanding of all the situation, I performed a CBCT.
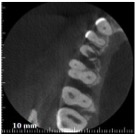
At this point, I wondered:
“Do I really have to surrender to a defect which is perfectly treatable, and also clearly visible, thanks to magnifying goggles or a microscope?”
After all, Heithersay worked before 1999, when enlargements and microscopes weren’t that common, as well as 3D teeth scans. And if you read the paper where he describes the technique he used, you’ll shudder. With such an antediluvian technique, I’m surprised he’s had such a high success rate!
As you’ll be able to see in this video, my idea totally made sense. With a microscope and a CBCT, treating such cases surgically is absolutely feasible and, let me tell you, not even that difficult.
You see?
Do you think this tooth will last less than 3 years? I can tell you “no” already, since this treatment turned 3 years old in September 2016 and the tooth is still perfectly healthy, both clinically and from the X-rays.

You don’t need to practice this technique 1000 times to be successful, and this is confirmed by the fact that this tooth was the first one for me.
Since then, I carried out four more class IV resorptions, publishing the clinical records first on the Journal of Endodontics and then on the Italian “Giornale Italiano di Endodonzia”, and I had previously won the Lavagnoli Award at the Italian Society of Endodontics, presenting these 4 cases.

In the meantime, I used the same technique in at least 5-6- class III or II cases, while I restored surgically other 3 or 4 cases (I don’t remember how many, right now).
This teaches us two lessons:
Firs: external root resorptions are not rare, but rather difficult to diagnose in their early stages, because they look like cavities.
Second: if you know what you’re doing and you use your brain, you don’t need to go through extraordinary experiences or attend dozens of courses for years, before actually practicing some new techniques.
I went from total idiot in 2011 to great expert, in just two years and after two cases!
There are still many aspects to consider about external root resorptions. I’d like to talk you you about how I’m thinking about proposing a new classification of the problem, based on therapy options, and I’d like to show you more videos about it.
But since this is not a course on this topic, but just a hint I wanted to give you, I hope you were intrigued, and I suggest that you keep following us, since you’ll see pretty exciting stuff!
Stefano