Two days ago a colleague asked me publicly on Facebook for advice on this case

The question was whether, in my opinion, fixed rehabilitation on implants could be performed. This article, and especially the video that follows, are intended to be my suggestions to that colleague and anyone else who might find them useful.
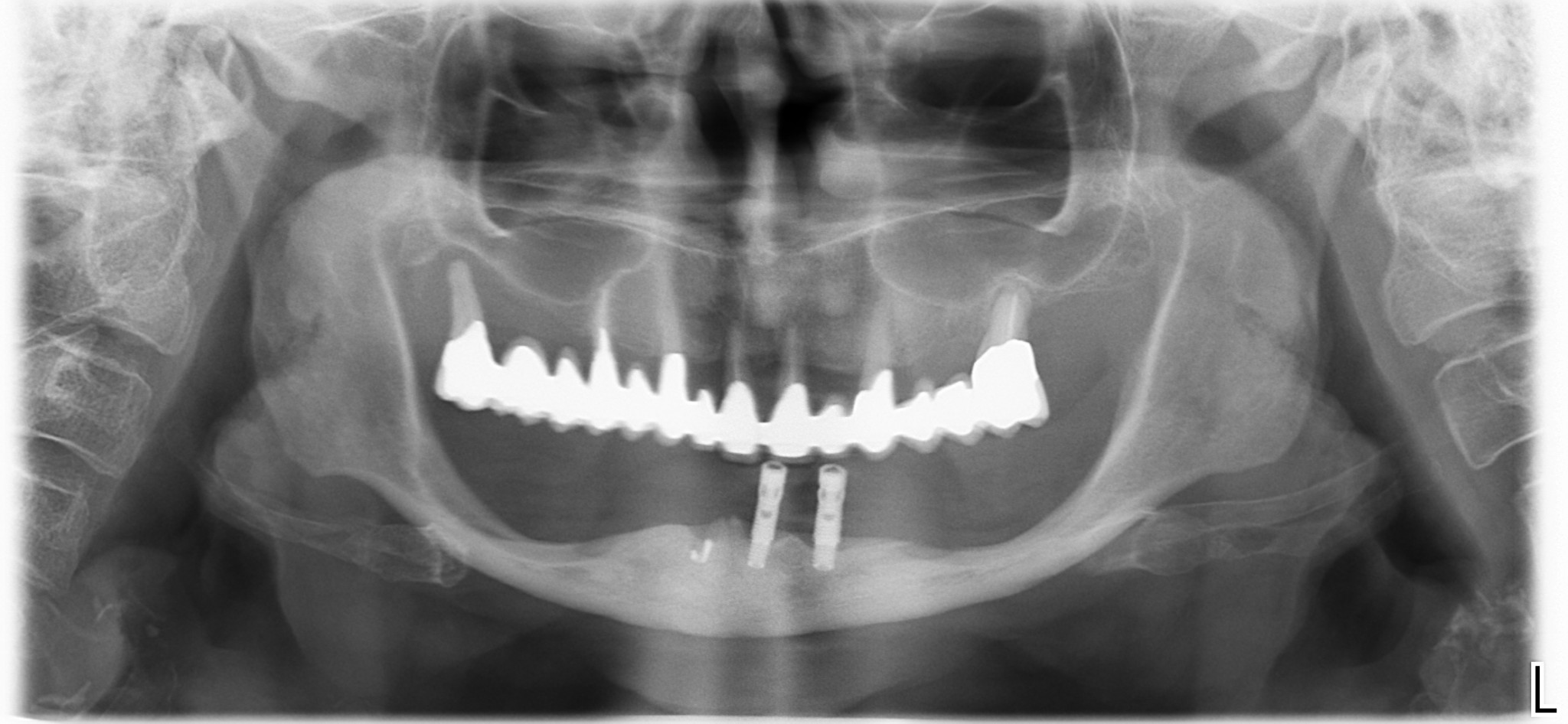
We will talk about the treatment of this patient of mine, treated five years ago, which seems to me very similar to that of the colleague.
In the meantime, I would like to make a comment on a topic that is very important to me but which I know is still very controversial in the dental community: standardization.
Fortunately, most colleagues are beginning to accept that operative (in this case surgical) procedures and techniques should be standardized and based on the best available scientific evidence.
Since the evidence in the literature, on long-standing topics such as implantology, is usually unambiguous and there are position statements and indications from scientific associations on various topics, these should be used to define one’s own operative protocols.
Discover the course "Simplification in full arch rehabilitation".
To give an example, back in 2012 the EAO stated that there seems to be no reason to place more than 4 or 6 implants in the rehabilitation of an arch and that treatment with 4 implants was, even then, a well-documented solution… ergo there is no reason to place more than 4 implants. Therefore, the rehabilitation of an edentulous jaw will be an all-on-4, always and in any case… unless there are absolute contraindications to implantology, which also include, of course, economic insolvency.
As you can see, however, in the space of one paragraph we have gone from clinical and operational indications to a DECISION-MAKING protocol, put another way, to a DECISION-MAKING STANDARDIZATION, and it is precisely this that many colleagues still cannot accept.
They want to evaluate, consider, assume, and balance… a thousand factors whose influence on treatment success, however, is not reflected in the scientific literature.
Therefore, they want to know the thickness of the bone (which is obvious in such a case), the age of the patient, the years spent with dentures, and even his dexterity… I wouldn’t be surprised if someone also went to assess the morphotype of the skull, the chewing cycles, the posture of the back, or the support of the soles of the feet on the floor 😱.
Sorry but this has no influence on the optimal treatment, which remains: four straight intraforaminal implants with 12 teeth screwed on top.
The doctor must understand that mistakes are right around the corner, especially in stressful situations, and standardization is the best way to minimize human error.
Now that you know how I feel about (almost) all the edentulous jaws in the world, I think it’s time to take a look at my surgery from 5 years ago, which someone might find useful… and you know what? Today, 5 years later, I would have done exactly the same movements… in the same order!
The same thing happens in hospitals and high-level surgery rooms where, for some 15 years now, standardized guidelines indicated by checklists and flow charts have been followed, thanks to the work of enlightened colleagues such as Pronovost and Gawande.
Discover the course "Simplification in full arch rehabilitation".Well, actually, thinking about it, I would have changed two small things, because remember that STANDARDIZATION does not mean immobilism but continuous refinement of procedures based on new evidence.
See you soon!