I’m sorry, but even if you don’t devote yourself to surgery, you’ve got to be able to perform a CLINICAL CROWN LENGHTENING anyways.
Or rather, in your practice, where you work with several colleagues, someone must be able to carry out a clinical crown lengthening in 30 minutes.
It’s a fundamental procedure in order to recover teeth, which were severely compromised by a carious lesion or by fractures, extended under the gingival margin. And please, take no offence, but I can’t help stating that recovering teeth compromised by cavities is absolutely the basis of operative dentistry.
Therefore, if you cannot enumerate this procedure among those carried out in your practice, it means you can’t carry out basic dentistry correctly; but since people, luckily, request high-quality basic dentistry treatments more and more, and ask less and less for dentures and full-
arch bridges, you’ll see your practice start running out of patients. And when you’ll be tempted to blame the economic crisis and low-cost clinics, remember these words and LEARN TO PERFORM A CLINICAL CROWN LENGHTENING ( or partner up with a skilled periodontist!!!).
Now, let’s start with the basics: DIAGNOSIS AND THERAPEUTIC TREATMENT PLAN.
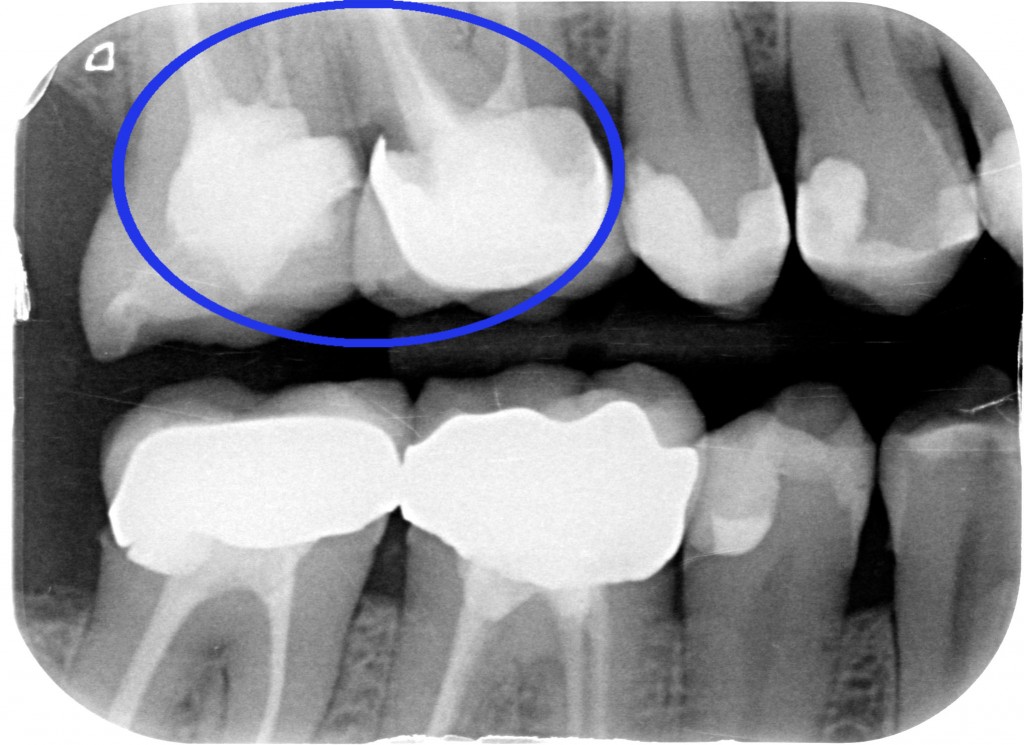
Academically, we could say: SECONDARY CARIES ON UPPER RIGHT FIRST MOLAR, PREVIOUSLY RESTORED THROUGH METAL CERAMIC CROWN.
But what I am saying to myself is “Whoever made that crown should have performed a clinical crown lenghtening, but he either didn’t want or didn’t know how to do it. So he didn’t manage to handle the distal preparation margin!!! So, some decayed tissue was left, or the margin wasn’t sealed correctly and thus…THE DIRTY DEED HAPPENED!”
Even though the patient wasn’t in pain, we gave him a full exam, which includes two posterior bitewing radiographs, so we noticed the problem. We’ve got to solve it, now. We could do three different things:
- Making the same mistake as my colleague had…mmmhhh, maybe not. Otherwise the patient will go look for a third dentist.
- Extracting the tooth and placing an implant…we might talk about it, but as a periodontist, I’d rather not.
- Perform a clinical crown lenghtening, which HARDLY takes THIRTY MINUTES (!!!) and then restore the element with a correct check of prosthetic margins.
If you have a fourth option, please write it as a comment below.
The apical repositioning of periodontal tissues will allow us to:
PROPERLY PERFORM A CORONAL PRE-TREATING

PROPERLY PERFORM A RE-TREATMENT OF THE ROOT CANAL, BY ISOLATING THE AREA WITH A DENTAL DAM

PROPERLY CARRY OUT A PROSTHETIC RESTORATION
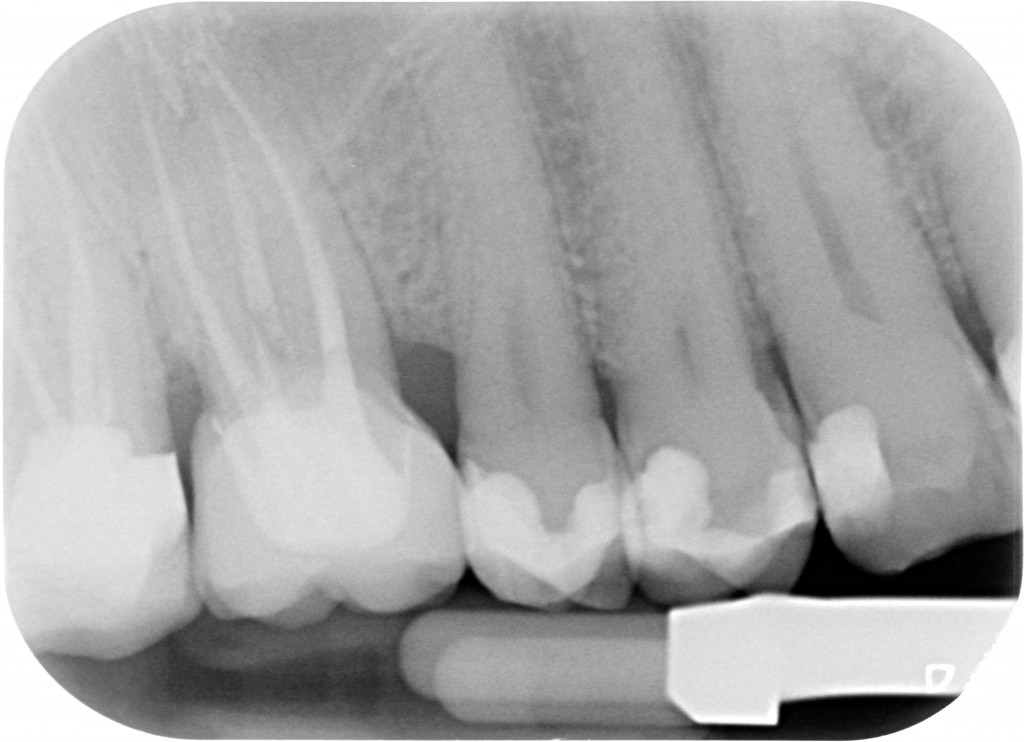
“Hey hey, check out what that guy did?! A notch on the back tooth!!”

Well, my friend, the bur needs to pass through the two teeth, so if the two roots are too close to each other, you need to create a space for an interdental papilla which isn’t in distress, where you may place a retracting cord (or, even better, two retracting cords) while you make the impression. Then yes, I’ll admit it: a couple of notches, here and there!
PS: “clinical crown lenghtening” doesn’t mean opening up the papilla, milling the interproximal bone a little and then stitch it all up! Technically, that’s called “creating a periodontal iatrogenic defect”.
Let’s now see this surgical technique.