Let’s go on with the fundamentals of soft tissue management in oral surgery.
In the previous article we went through the vertical incision in the posterior mandible and now you are ready to know what comes out when you perform a vertical incision in the maxilla.
Even if you think it’s bullshit and these could seem trivia, I really think there are a few things that need to be cleared up before performing surgery with a good awareness.
Have you ever heard Professors tell their students that a coronally advanced flap, aimed at root coverage, causes a shortening of the buccal sulcus?
I have! A lot of times! But the sulci of my patients don’t shorten… at least when I perform muco-gingival surgery (that is one of the most important topics in soft tissue management).
Instead, they shorten as hell when I perform bone regenerative surgery. However, in both cases I take a flap and I pull it down.
Thake a look at this fifth sextant as an example…
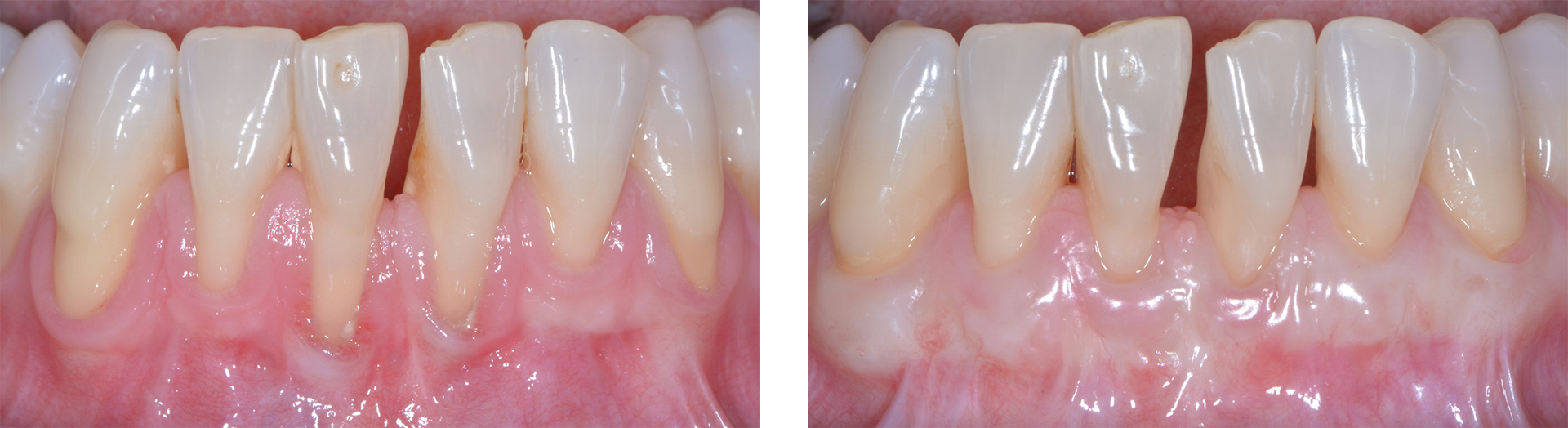
… no buccal shortening! And this second sextant…

Again, NO WAY, no sulcus shortening!
There is a huge difference, indeed, between the two ways we move coronally the flap when we either want to cover a root or when we want to cover a bone graft. To be both a good periodontist and a good implantologist it is mandatory for you to understand the anatomy of the zone. As a periodontist you will go one way as an implantologist you will go the other way. And imagine that in some surgeries you will be supposed to work in different ways depending on the zone or to the aims you have. And only then, when you become a Superperioimplantologist, you will be allowed to say “I’m good at soft tissue management”.
But now let’s take a look at the simple anatomy of the maxillary sulcus.
As you see in the photo, when the incision in the vestibule is made in a full thickness manner, you meet sequentially:
- The mucosa
- The sub-mucosa
- The muscular tissue
- The periosteum
And you stop over the bone.
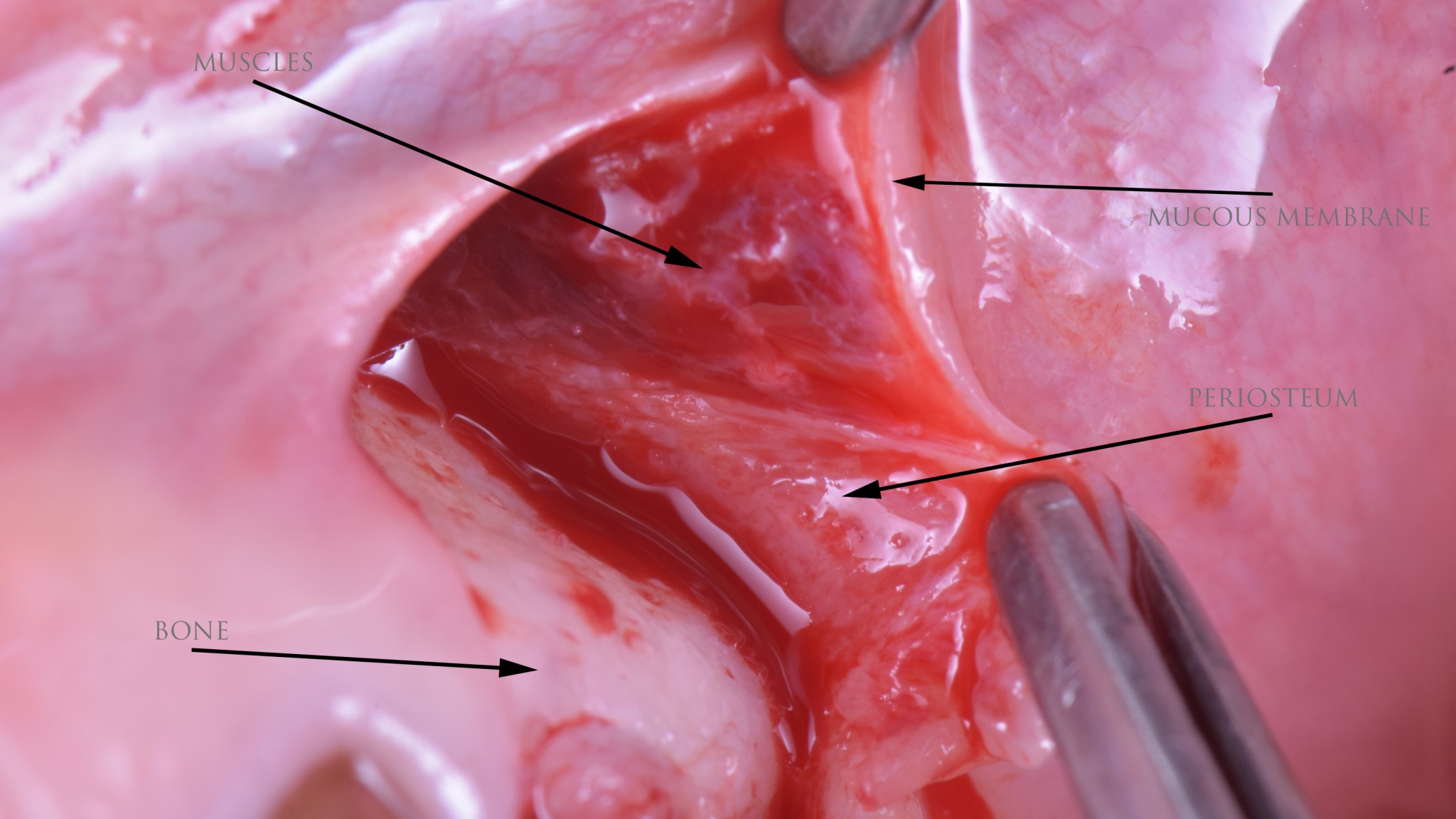
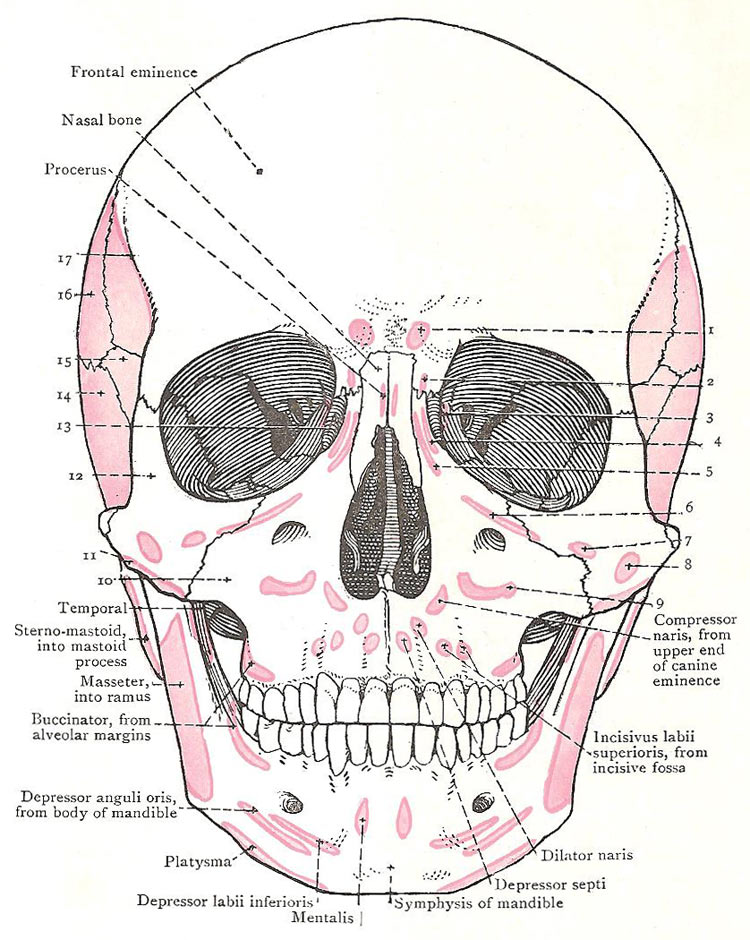
The muscles you find there are of different kinds, in the anterior zone there are some mimical muscles like the Incisivus labii superioris, further back there is the buccinator. Remember, we have already talked about this last one /about the latter.
One of the notions I’m showing you in the video below and that you need to definitely know is this:
The muscular tissue you have seen in the previous pic is STRONGLY attached both to the sub-mucosa and to the periosteum.
Remember this… we’ll need this information later on.
Certainly, you have performed some bone augmentation in the upper jaw or, at least, you have seen one. When Increasing the underlying bone volume, you’ll need more “fabric” to cover it and, considering that the palatal tissue can’t be advanced, the technique we all use is to cut the buccal periosteum and ”extend” the flap, doing, more or less consciously, two things:
- We dissect the fibers of the muscles, which, In that way, lengthen.
- We “stretch” the mucosa and the sub-mucosa that are deliciously elastic.
Pulling down the mucosa, this takes with it the muscular fibres that are STRONGLY ATTACHED TO IT (it will be clear in the video) and there the sulcus shortens, because these fibres will attach lower/futher down. And you will get the typical aspect of fatty, squishy and mobile stuff that goes all the way to the palatal area of the crest.
As an example, look at this case – four months after a GBR procedure…

Here is the misunderstanding: If you use the same approach for the mucogingival surgery, you’ll have AN UNSIGHTLY AND DETRIMENTAL SHORTENING OF THE SULCUS, with awful muscular fibers that will attach more coronally and will pull on the flap you have just repositioned.
And this flap is not anchored to the palatal one with a “super performing” double layer suture (as in GBR), but it is maintained in place by micro sutures anchored on little papillae and lies, for the great majority, on avascular root surfaces. It is not so strange, I guess, that surgeons who use this approach do not love the muco-gingival surgery: results will look like crap and anything but fulfilling!
When you perform a mucogingival surgery YOU MUST DETACH the muscular fibres both from the periosteum and from the submucosa. In that way, the muscle will pull back in the depth of the sulcus and you will pull down only the mucosa and the submucosa?.
No sulcus shortening… no muscular tension on the flap… no fatty stuff in the coronal position.
To show you everything and contextualize these concepts in both everyday and advanced surgery I’ve built an online course about soft tissue management. The course consists only of surgical videos.
8 hours of commented surgery
14 lessons
20 surgical interventions (what the fuck? 20 surgeries in 8 hours? Well, you know, if you can work, you work fast .. we have already stated this!)
You’ll find everything you need to handle soft tissues, not only to stretch a flap to cover a graft! This is the topic of a single lesson. The rest is something no one tells you.
The course is having a huge success in Italy so I have decided to translate it in English!
You have the opportunity to get the EARLY BIRD PRICE only till the 31st of March, saving 244 euros!! Discover more about the course here
Very energetic blog, I enjoyed that bit. Will there be a part 2?
Neat blog! Is your theme custom made or did you download it from somewhere?
A theme like yours with a few simple adjustements would really make my blog stand out.
Please let me know where you got your theme. With thanks
It’s a custom made by Etinet srl, our web design agency
Massimiliano
What’s Happening i’m new to this, I stumbled upon this I
have discovered It absolutely useful and it has aided me out loads.
I’m hoping to contribute & aid different users like
its helped me. Great job.