Speaking about delayed implant positioning, a scientific article says “…This delay, combined with ridge resorption following extraction, may contribute to several problems. Insufficient available bone for ideal implant placement and prolonged treatment time are two common difficulties… immediate placement of dental implants into extraction sockets… can eliminate the above-mentioned difficulties.”
What’s your opinion? Would you consider it a modern perspective?
Definitely not, it’s pure bullshit deriving from the ignorance on biological mechanisms behind post extraction healing, that used to affect dentists back in the Nineties and at the dawn of the new millennium.
The belief that immediate implant positioning could prevent bone resorption after extraction was widespread in the dental community when I was graduating in 2004, but it was proven wrong by some scientific studies by Araujo, Lindhe and Botticcelli published in 2005 and 2006.
I still remember the first time I heard this concept. It was during a congress of an Italian dental company. I remember it very well, because the paradigm shift was dramatic.
Let’s start from the very beginning: the 2005 study by Araujo & Lindhe:
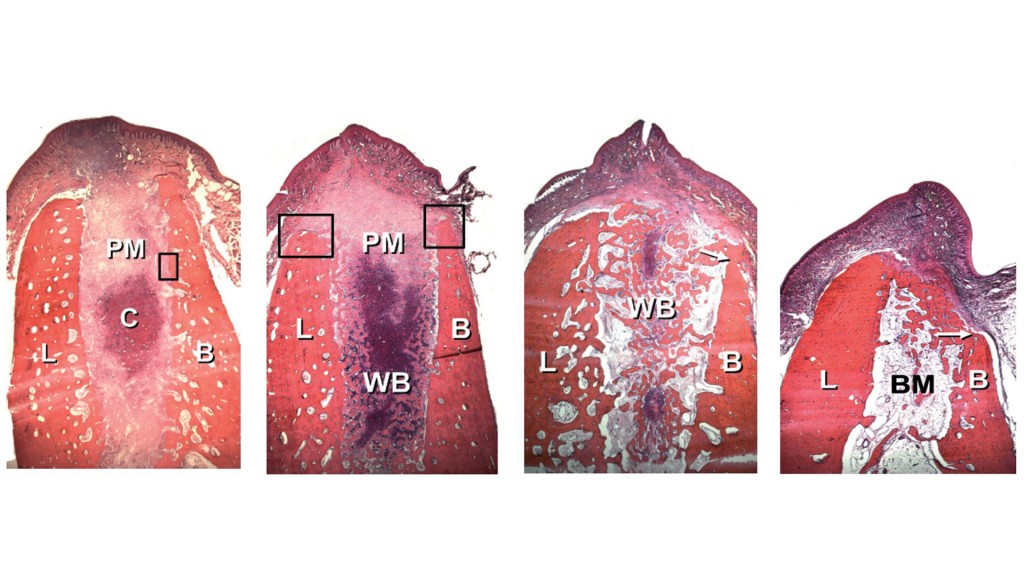
Even if we ain’t pathologists I guess we both are able to interpret the images above. The first one refers to a dog socket one week after extraction, the last one to a dog socket eight weeks after extraction. This histological experiment shows that the alveolar process RESORBS itself, above all horizontally (but also vertically), and in particular from the buccal point of view.
Now some “smart” readers will refer directly to the article and will reply:
“You are a dummy because in that experiment full thickness flaps were raised, and this was the reason why the alveolar bone resorbed… oh and, by the way… we’re talking about dogs, not men!”
And I, who constantly question myself when I get a criticism, am going to dive deeper into the topic by studying more articles, only to discover what happens to men when they undergo extraction WITH NO FLAP LIFTING; and I think I will find more or less concepts like these:

Summarising: the volume of the ridge after an extraction in the middle part of the edentulous zone resorbs ON AVERAGE by 15% within 2 months (that is quite similar to Araujo findings, isn’t it?), by 40% within 6 months and by 50% in 12 months.
“Screw that, I’ve got a patient to whom I extracted a tooth and after some months he showed no loss of volume!”
Buddy, this is no less bullshit than stating “my grandma smoked for 70 years and she didn’t get cancer!”
These things have a NORMAL distribution, which graphically is something like this:
The majority of cases are located here:
And resorb 50% of volume in 12 months. Luckily, only a small number are here:
And they resorb much more. Finally, unfortunately only few are here:
And they resorb very little. Obviously when we extract a tooth and insert an implant straightaway we, smart doctors, have to cautiously foresee the patient will fall in the middle of the Gaussian curve, where the great majority of patients fall after a tooth extraction.
“Ok, I’ll put a screw in there immediately and everything will be ok!”
NOOOOOOOOOO!
Look what Botticelli demonstrated in 2006:
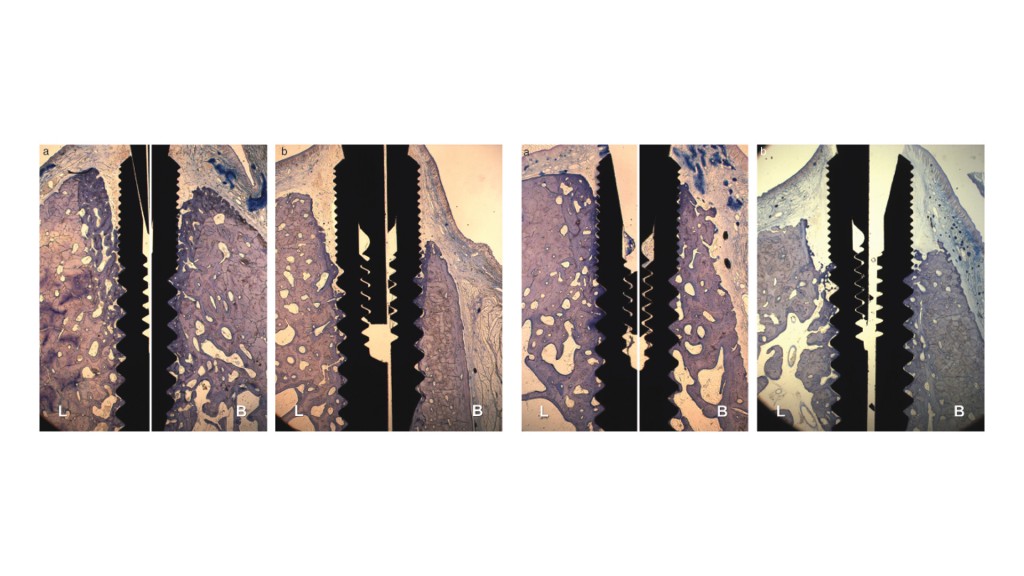
The first two images show you what happens after 2 months if you place an implant in an artificial “hole” made in healed bone compared to what happens doing the same thing in a post-extractive socket; the last two show you the same after 4 months. As you can see, after extraction, alveolar bone resorbs in the same way as if the implant had not been there, instead, in an “artificial hole” case, even if a flap was lifted the resorption was irrelevant!
And now take a look at what excites me the most in these images:
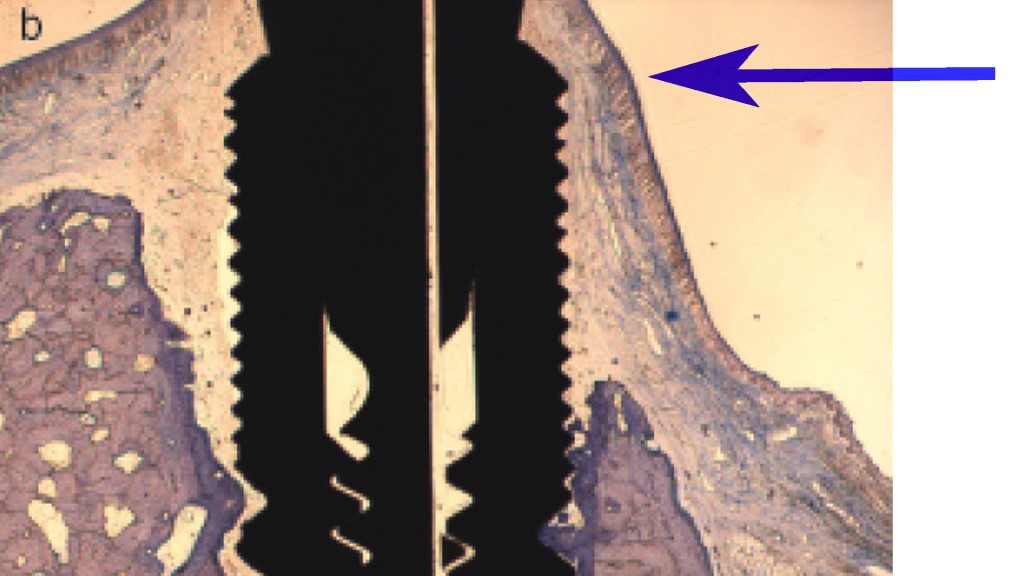
A very thin and unstable layer of gum, for some reason, lays glued to the healing screw and to the coronal part of the implant which now is completely out of the bone. That is to say, if you lookat this implant from buccal you will see a narrower recession compared to the one you would see with the extraction alone, BECAUSE THE HEMIDESMOSOMES remain attached to the titanium. But you will have anyway:
- A certain recession
- A bad stability over time, because of the thinness of the tissue
- A volume reduction with, as a consequence, a concavity in the pink aesthetic apical to the crown that will cause an ugly shadow
- The grey colour of the titanium that will be visible though the tissues
In other words, you will get this:

Even if the ceramic crown is quite pretty… the rest is an eyesore, isn’t it?
I’ve already gone through the protocol to be used in the management of post-extractive implants in the aesthetic zone elsewhere, here I’d like to give you some advice about the treatment of already atrophic edentulous zones. I mean how to treat 90% of delayed implant cases we meet in our practice, so as to fix the unavoidable lack of volume. Let’s say… the ones who fall in the middle of the curve. With the ones on the right part of the curve, you can go flapless instead; with the ones on the left part, you will have to increase the bone.
Consider that this tooth was removed WITHOUT A FLAP and… 50% horizontal volume reducion!

The technique I’m going to show you in the video has been described in a recent article by Stefanini et al. and is really simple! If you are thinking “Who on earth would give a shit? It’s in the posterior zone!”, do me a favour, don’t watch the video because we are two worlds apart! (sorry if the song underneath the video is Italian. It’s about Bologna, the city of the master who invented this technique).
And now let’s get down to work!
Federico
P.S. remember to subscribe the newsletter not to lose the new contents!!!
It works quite well for me
Thank you for your blog article.Really looking forward to read more. Will read on…