Our co-worker Lodovico is used to taking advantage of me, in the Clinic halls, to solve all the doubts he has after attending courses, as if I were Morla the “ancient one” turtle from the The Neverending Story.

About one month ago, back from some sort of course, he asked me ironically:
“By now, in every course they say that putting down implants is not the most difficult thing, SOFT TISSUE MANAGEMENT is, instead. Can you tell me what the hell is this soft tissue management? You take the flap and stretch it… Big whoop! Very difficult thing!”
Actually, the soft tissue management concept could be tough to understand because in the past the challenging goal of implantologists was to succeed in placing implants and make them stay there in the bone.
If the bone was not enough we had to “create” it in some way and to cover the bone… we were supposed to stretch the “blanket”.
As a consequence today’s mindset is:
The height of self-satisfaction was to be able to release the lingual flap. Consider that my first master, during my first implant course 13 years ago, told me:
“we don’t release the lingual flap any more, because it’s too dangerous!”
Now we know that the lingual flap can be stretched without any risk and in a very simple way, we know that reconstructive techniques, as difficult as they may be, work and we have short implants at our disposal which work too.
We can say that nowadays, even if the implant is placed by Mikey Mouse, it has a 90% chance to hold in there (if it’s placed by an expert surgeon the odds become more than 98%) SO THE GOAL MUST BE BROUGHT TO THE NEXT LEVEL!
Let’s go back to Lodovico’s question. My answer was:
“Take a look to this XR, what do you think? Is this implant healthy?”
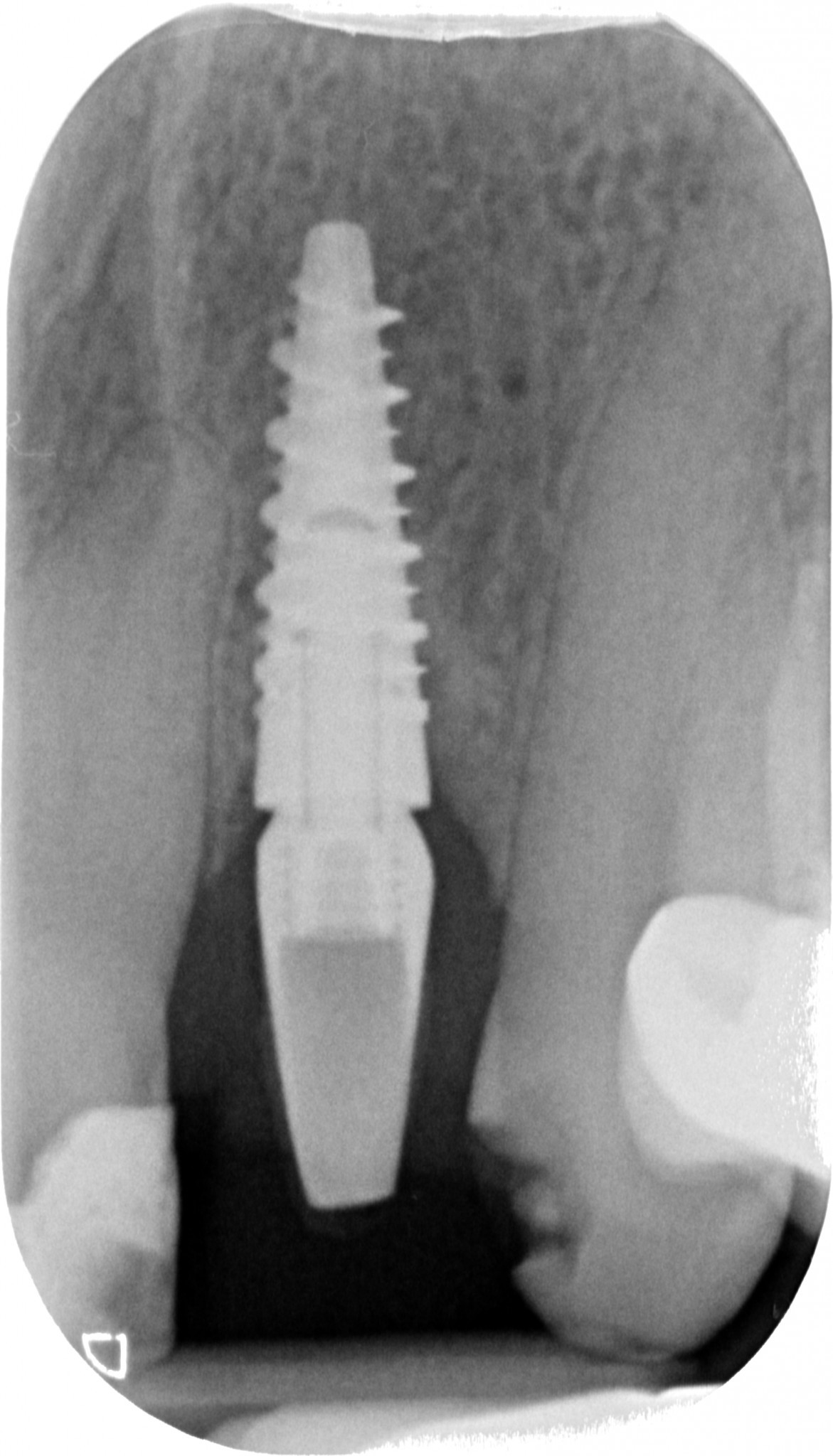
Perfect I’d say, not the least sign of bone resorption. I guess you will agree with me.
Miss Rosetta underwent this treatment in her old dentist’s practice. As he bonded the permanent crown, 6 months ago, she started complaining about a continuous dull pain. The dentist, I dunno why, removed the crown and bonded the provisional again.
The symptom kept on bothering her, Rosetta kept complaining. Running out of ideas, the colleague decided to resort to…
THE GOLD TECHNIQUE… that I saw used plenty of time as a last resort during my early years, when I was working as a consultant:
“I’m sorry madam, everything’s ok here, you are healthy”

For once, let me play the role of the serious and polite practitioner.
The physical examination highlights:
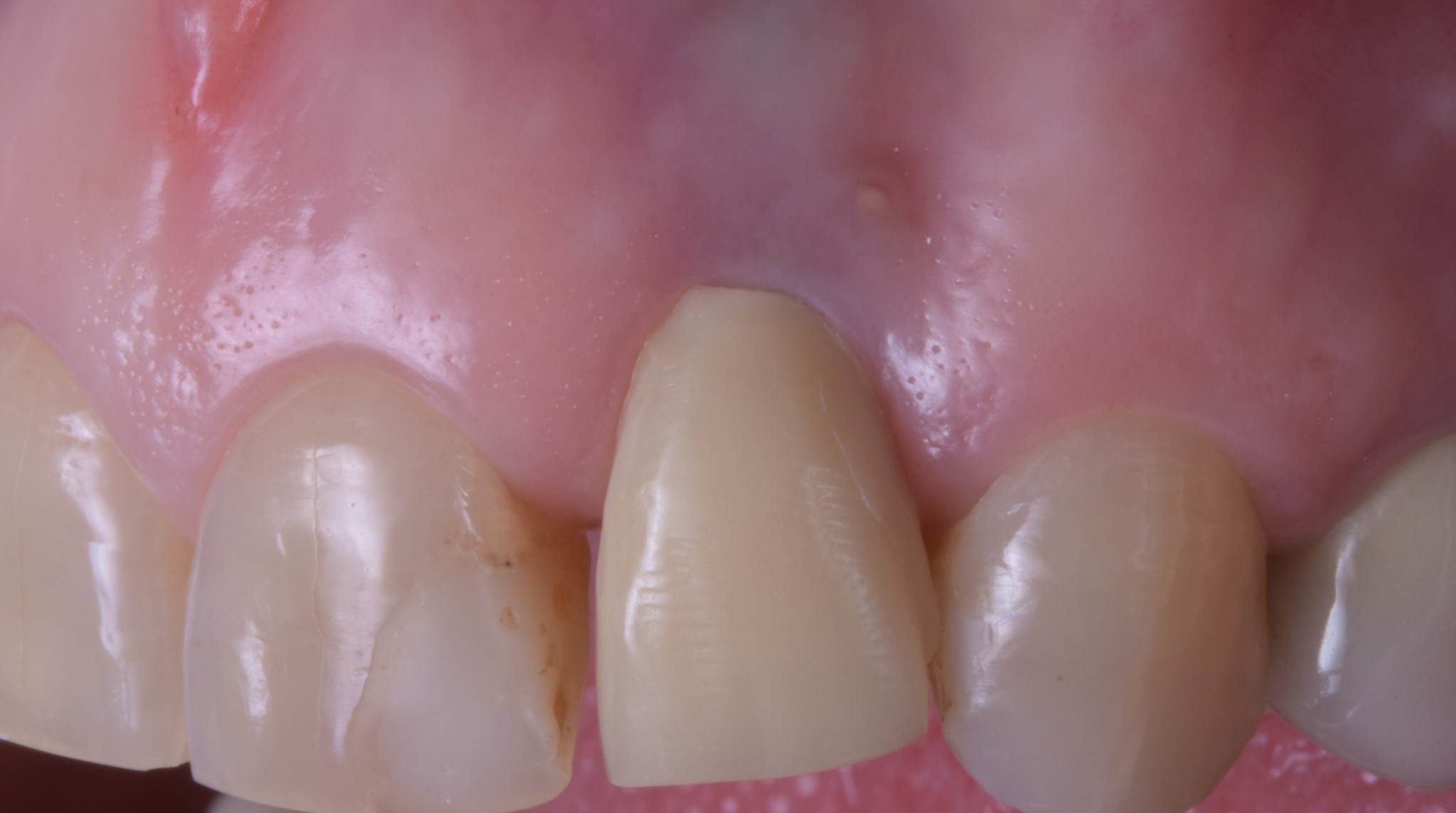
- Buccal fistula related to implant-supported 2.2
- Aesthetic result… (I’m sorry but I must be me again) shitty!!
And please don’t tell me “you can’t judge this case, because you don’t know how tough it was”, because until 1 year ago the patient had her tooth in place which was removed and replaced with an implant because of restorative issues, neither because of infective nor periodontal ones. That means that a post-extractive implant was placed in a healthy socket. I’m quite positive to say that difficult cases are a whole different story. Dear Lodovico, here is an implant that allows the patient to chew, with a very beautiful XR bone aspect (later on I’ll explain you the fistula’s cause), which properly fills the “hole” left by the extraction, but with an AWFUL SOFT TISSUE MANAGEMENT!
“Can you see now, Lodovico, what I mean when I talk about soft tissue management?”
An implant-supported tooth, today, should have this aspect.

Or this one, if you want an example from the frontal area.

Especially if the tissues were originally optimal and healthy.
But let’s go back to Rosetta’s fistula. You must respect and manage the soft tissues also in the prosthetic phase, not only in the surgical one. If you handle biology as you can see here below, a fistula is the least serious problem you will be likely to face.



Look at:
- The polishing of the abutment
- The cleanliness of the abutment close to the bone
- The precision of the provisional
- The invasion of the biological tissues by the prosthetic margin, leading to the impossibility to manage the bonding interface.
In such a condition, your best option is to use THE GOLD TECHNIQUE… the problem is that, it’s just a matter of time, the patient, who is not dumb, will get rid of you and start looking for someone able to solve their problem.
And this is exactly what happened: Rosetta came to my Clinic asking for a solution.
I solved Rosetta’s pain and fistula in very few days, by simply achieving a good provisional rehabilitation.

And once the gingival tissue was healthy again, I was able to fix the aesthetic issue thanks to a 1-hour surgery. The surgery lasted for one hour only because I also recorded a terrific 4k super-video in which you’ll be able to see even the cells of the patient. Without the video I’d have performed the surgery in half an hour. Not (only) because I’m fast, but also because the surgical technique is really smart.


I’m showing you the 7-day-healing for two reasons.
- The beauty of a surgery must be evaluated at seven days, if you wait for 2 years, also a shitty surgery leads to a satisfying outcome.
- The patient underwent the surgery 7 days ago and I don’t have more recent pics, but I think you will agree with me that after such a pretty healing it will be very unlikely to encounter any surprises.
As you can see, we have fully fixed the soft tissue volume deficit left there after the previous rehabilitation and…
we have laid the foundations for a new rehabilitation, which can be called worthy of today’s state of the art.
Now, if you are a soft tissue management expert, I thank you dearly for your kind attention… feel free to click on the red cross in the upper left part of the screen. If you are not an expert yet, you do have a choice:
1) You can become a master of THE GOLD TECHNIQUE, learning how to fool your patients… and soon enough you will see them running away from your practice.
OR
2) You can become a skilled master in soft tissue management and learn the concepts you can find in my online course
But let me list what you will find in my course:
- Only commented surgical videos explaining all the steps of the soft tissue management techniques
- Only high definition videos with the right frame
- The technique which will enable you to stretch the lingual flap in few seconds and without any risks
- The releasing techniques both for the maxillary and the mandibular flaps you need in reconstructive surgery
- All the lies they told you about connective tissue graft and the right updated techniques
- The post-extractive implants protocol to spare your patients Rosetta’s outcome. Some people don’t know yet that bone resorbs after extraction, even if you put the implant immediately!!
- All the techniques you need to cover gingival recessions
- All the techniques you need to increase keratinized tissue around implants
- How to build a new gingival anatomy with new papillae, also in posterior zones
- To cut a long story short, all you need to deliver super aesthetic results to your patients and, above all, not to make the mess you have seen in this article
What you won’t find in the course
- My ugly face explaining you theoretical out-of-context topics
- Slides with schemes, graphs and scientific articles
- Blood-caked surgical field where nothing is clear
- Wrong frames
- Big frames where you see the whole face of the patient but are unable to look at what’s going on in the mouth.
If you want to know more before buying, you can read the course program here.
Now go straight to the course: When the going gets tough, the tough get going!
I am now not certain where you’re getting your info, however good topic. I needs to spend a while finding out more or figuring out more. Thanks for magnificent information I was on the lookout for this info for my mission.